
An Ebola epidemic is underway in the Democratic Republic of Congo, caused specifically by the species Bundibugyo (BDBV, Orthoebolavirus bundibugyoense), one of the four types of Ebola so far identified as pathogenic for humans. On 16 May 2026, the Director General of the WHO, based on the provisions of the International Health Regulations, declared the situation a public health emergency of international concern (PHEIC, Public Health Emergency of International Concern). The WHO was keen to clarify that this emergency it is not the same as a pandemic emergency (pandemic emergency), signals an emergency requiring international coordination, but does not imply a high risk for the general population outside the affected region. As regards theItalythe Ministry of Health confirmed via circular that, for purely preventive purposes and in accordance with WHO recommendations, surveillance protocols have been activated for the monitoring of travelers arriving from the areas affected by the outbreak.
In the Democratic Republic of Congo they are currently registered (data May 19 from the US CDC) 34 confirmed cases and 536 suspected cases, with 105 deaths. In Uganda 2 cases were confirmed, including 1 death, both in people who had traveled from the Democratic Republic of Congo. The first currently known suspected case is a healthcare worker who reported the onset of fever, hemorrhages, vomiting and severe malaise on April 24, 2026, and died in a medical center in Bunia, the capital of the province of Ituri. However, the total number of cases may be underestimated due to the complexity of surveillance in rural areas and the similarity of symptoms to other endemic diseases, such as malaria.
What are Ebola viruses and what are the types
“Ebola” refers to a group of viruses from the Filoviridae family, a RNA single filament, recognizable under the microscope by their filamentous form from which the family takes its name. The first documented outbreak dates back to 1976 in two almost simultaneous epidemics in Sudan and in the then Zaire (now the Democratic Republic of the Congo), near the Ebola River from which the virus takes its name.
The US Centers for Disease Control and Prevention and the WHO recognize it within the genus Orthoebolavirus today six speciesbut only four cause confirmed disease in humans and three of these are capable of triggering large epidemics.
The Ebola virus (species Orthoebolavirus zairensehence the acronym EBOV) is the one discovered in 1976, responsible for most historical outbreaks and the 2014–2016 epidemic in West Africa that caused over 11,000 deaths. The disease it causes is called Ebola Virus Disease (EVD) and it is the one with the highest lethality – up to 90% in untreated outbreaks, on average 50% according to WHO.
The Sudan virus (SUDV), identified in the same 1976, causes the Sudan Virus Disease (SVD)with historical lethality between 41% and 70% depending on the outbreaks. The latest species with documented epidemics is the Bundibugyo virus (BDBV), first isolated in 2007 in Uganda. Cause the Bundibugyo Virus Disease (BVD)with a lower historical lethality than other strains of around 25–40% according to cumulative WHO and CDC data.
The Taï Forest Virus (TAFV), however, caused a single human case in 1994 in Côte d’Ivoire, in which the patient survived. The other two species of the genus (Reston and Bombali) have never caused confirmed disease in humans.
How it is transmitted: origin and human contagion
The “natural reservoir”, i.e. the animal that hosts the virus without getting sick and from which the virus jumps to humans, is suspected to be the fruit bat. Spillover to humans usually occurs through contact with infected primates, forest antelope or bats, alive or dead, in forest areas. There is no evidence that mosquitoes or other insects can transmit the viruses that cause Ebola disease.
One reason Ebola never spread globally, as SARS-CoV-2 or influenza did, is its transmission mechanism. Ebola is not transmitted through the airthat is, it does not travel on droplets or respiratory aerosols like an influenza virus does. To move from one individual to another you need a direct contact with the body fluids of an infected person who has already developed symptomsfor example through wounds, abrasions, or mucous membranes of the eyes, nose and mouth.
The documented potentially infectious fluids are blood, vomit, feces, urine, saliva, sweat, tears, breast milk, amniotic fluid, semen, and vaginal secretions.
Symptoms of Bundibugyo virus disease
From a clinical point of view, BVD is practically indistinguishable from other Ebola virus diseases. The incubation period (the time between contact with the virus and the appearance of the first symptoms) is from 2 to 21 days.
The initial symptoms are nonspecific and resemble those of a severe flu-like syndrome sudden high fever, extreme tiredness, muscle pain, headache, sore throat. It is the phase in which clinical diagnosis is most difficult, because in many endemic areas malaria, typhoid fever and meningitis also coexist with Ebola, which begin in a similar way.
The framework then evolves into a second phase with vomiting, diarrhoea, abdominal pain, skin rashes, changes in kidney and liver function. It is in this phase that the patient loses large quantities of fluids and electrolytes, and dehydration becomes one of the first causes of clinical impairment.
In severe cases, the hemorrhagic phase appears, the one that gave Ebola its media fame as “haemorrhagic fever”. The virus attacks endothelial cells, those that line the inside of blood vessels, and interferes with the coagulation cascade, causing internal and external bleeding. However, according to WHO, hemorrhagic manifestations are not as common a symptom as one might think.
The diagnosis is made through RT-PCR (the same technique used for SARS-CoV-2), antigen tests and genomic sequencing, the latter being fundamental for distinguish BDBV from other strains.
Cures, treatments and vaccine
Today we have effective tools against “classic” Ebola (species Zaire). On the preventive front, vaccines are approved Ervebo and the regime Zabdeno/Mvabea. On the treatment front, theFDA has approved two therapies with monoclonal antibodies which, by binding to the glycoprotein of the virus, prevent it from infecting human cells (Inmazeb and Ebanga).
No product has so far been authorized and proven effective against the Bundibugyo virus. The surface glycoproteins of the two viruses are different enough to make existing monoclonal antibodies, built on EBOV, largely ineffective on BDBV.
The treatment of patients with BVD is therefore based, today, above all on supportive therapy with intravenous rehydration with balanced electrolyte solutions, correction of sodium, potassium and calcium imbalances, blood pressure support in patients in shock, oxygen therapy and adequate nutrition.
Because the WHO has declared an international health emergency
Prior to the current outbreak, documented cases of Bundibugyo virus disease worldwide consisted of only two episodes. The first outbreak was recorded in Bundibugyo districtin western Uganda on the border with the Democratic Republic of Congo, from which the virus takes its name. The final balance, as reported by the WHO, was 131 cases and 42 deathswith a mortality of 32%the lowest ever observed for an Ebola outbreak up to that point. The second historic outbreak was declared on 17 August 2012 in the Eastern Congolese province, in the areas of Isiro and Viadana. The official WHO numbers speak of 59 total cases (38 confirmed and 21 probable) e 34 deathswith a lethality of 57%. The epidemic was declared over on November 26, 2012.
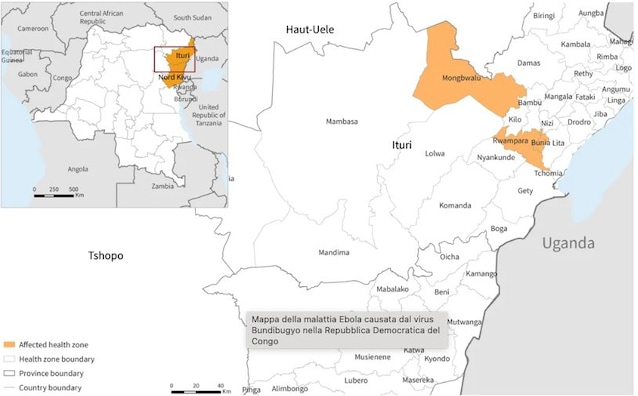
According to WHO investigations, the current outbreak originated in the Mongbwalu area, a mining area in the province of Ituri (northeast of the DRC) with a high traffic density, and then spread to nearby Rwampara and Bunia through patients who moved in search of treatment. The fact that Ituri borders directly with Uganda and South Sudan, together with the two imported cases registered in Kampala, prompted the WHO to declare a public health emergency of international concern (PHEIC). It is the same tool already activated during the large Ebola epidemic in North Kivu and Ituri between 2018 and 2020 and during the one in West Africa between 2014 and 2016.
There are four official reasons that led to this decision. The first is the size of the outbreak: as of May 16, there were 246 suspected cases, 80 suspected deaths and 8 laboratory-confirmed cases in three health areas of Ituri, in addition to the two cases in Uganda, which however appeared 24 hours apart from each other and without any epidemiological link between them, a sign that the viral circulation upstream is probably much wider.
A’analysis published on May 18 from the MRC Center of Imperial College London together with the WHO estimates that the real cases in DRC are between 400 and 800i.e. double or triple those officially reported. Furthermore, there are active propagation signalsinvestigations are also underway in other areas of Ituri and North Kivu, and four healthcare workers from Mongbwalu hospital died in just four days, indicating violations of infection prevention protocols.
The fourth motivation is the operational context: an armed conflict is underway in the province of Ituri which has generated 273,403 displaced people.